My son called from the hospital. When I arrived, the doctor said, “Chief of Surgery… he’s your son?”
My son called from the hospital. Dad, the doctor is refusing to treat me. He says I’m faking my symptoms to get drugs. When I arrived at the guar, the doctor’s confident expression disappeared. He lowered his voice and said, “Chief of surgery. I didn’t realize he was your son.” The call came at 3:47 a.m. on a Friday. While I was reviewing surgical schedules for the upcoming week, my son Ethan’s name appeared on my phone screen and my chest tightened instantly. Ethan was 22, a graduate student at State University 3 hours away. He never called at that hour unless something was seriously wrong.
Dad, I’m at Mercy General’s ER. His voice was strained with pain. I’ve been here for 2 hours and the doctor won’t treat me. He keeps saying I’m pretending to get painkillers. Dad, something is really wrong. It hurts so much I can barely stand. I was already reaching for my keys. What symptoms? Tell me exactly what you’re feeling. He took a shaky breath. It started around midnight.
Sharp pain in my lower right abdomen.
It’s getting worse every hour. I’m nauseous. I’ve thrown up twice. I have a fever. I tried explaining all of this, but the doctor just kept asking about drug history and looking at me like an addict. My hands went cold. Lower right quadrant pain, nausea, vomiting, fever, a classic appendicitis presentation. If it was appendicitis and they were ignoring it, his appendix could rupture.
That meant sepsis, peritonitis, possibly death. Who’s the attending physician? I asked. Dr. Vance. Dr. Leonard Vance. He barely examined me, did a quick palpation, hardly touched my abdomen, then told the nurse to give me Tylenol and discharge me. Dad, I’m not making this up. Something is wrong. I was already backing out of the driveway.
Don’t let them discharge you. Tell them your father is Dr. Garrison Mills, chief of surgery at St. Catherine’s Hospital, and I’m on my way. Do not leave that ER, Ethan. If your appendix ruptures because of delayed treatment, people will lose their licenses. I had been chief of surgery at St. Catherine’s Hospital for 8 years and a general surgeon for 23 years before that. I had seen every complication, every delayed diagnosis, every case of negligence that ended in tragedy. One thing that always angered me was when doctors allowed bias to override clinical judgment. Young men with abdominal pain were often dismissed as drug seekers, especially if they had tattoos or piercings or looked unconventional. Ethan had full sleeve tattoos, long hair, and a nose ring. He fit a stereotype some physicians used as an excuse to avoid doing proper work.
But Ethan was intelligent, compassionate, and never used hard drugs. He was finishing his masters in environmental science and volunteered at wildlife rehabilitation centers on weekends. The thought that an ER doctor had judged him on appearance rather than symptoms was unacceptable.
The drive to Mercy General took 2 hours and 38 minutes. I spent the entire time on the phone, first with Ethan to monitor his condition, then with colleagues to gather information about Dr. Leonard Vance. What I learned was troubling. Vance was 46 and worked as an ER physician for 15 years. Multiple patients had filed complaints claiming he dismissed symptoms and provided inadequate care. None led to formal discipline because the hospital quietly settled issues and the medical board never pursued them. Nurses reportedly described him as dismissive and quick to label patients as drug seekers without proper evaluation. One colleague, Dr. I.
Simmons, who had worked with him years earlier, told me directly, “Garrison Vance relies on his credentials and avoids thorough workups. He profiles patients by appearance. I’ve heard he’s especially dismissive toward young men.
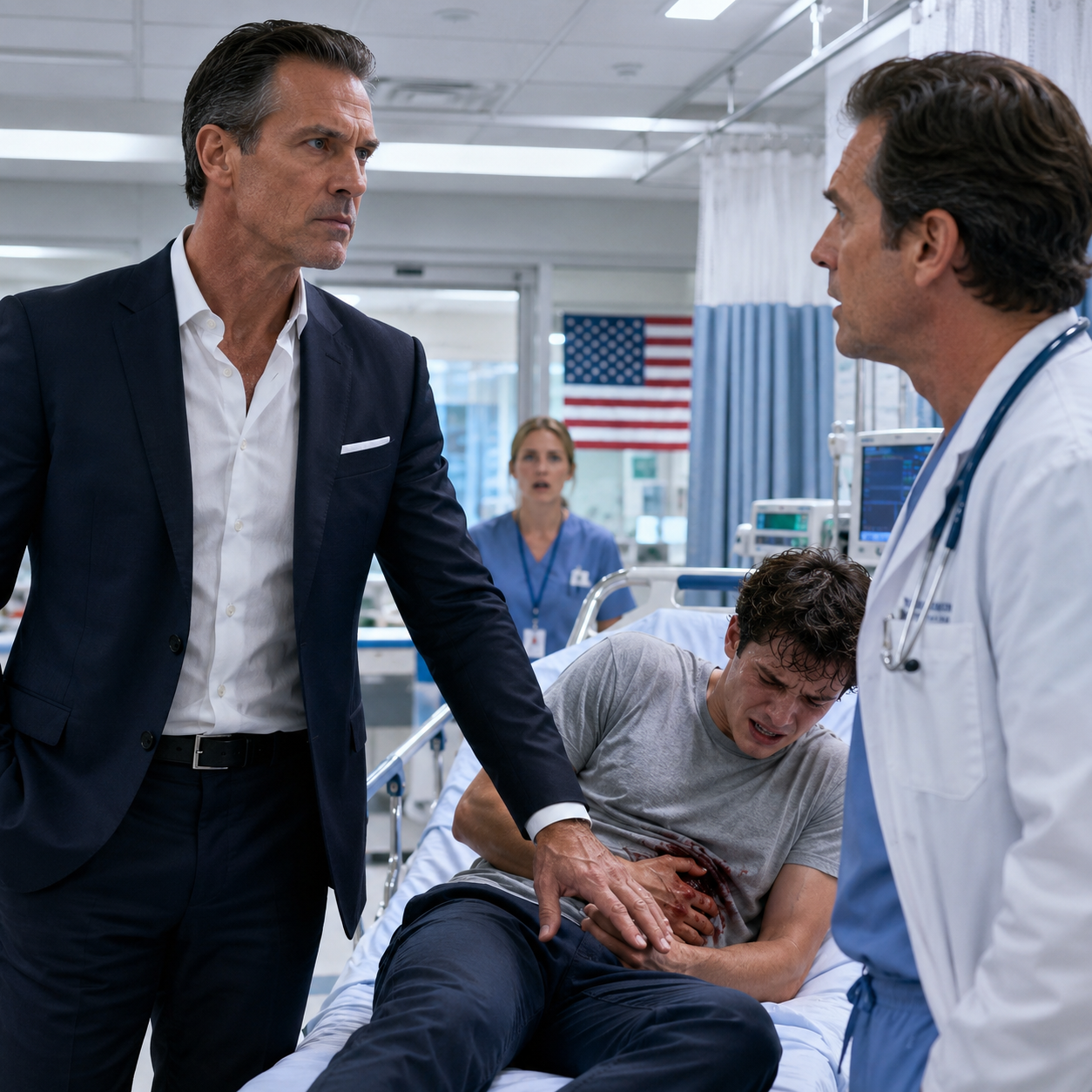
When I arrived at Mercy General at 6:31 a.m., Ethan had been in the ER for nearly 5 hours without meaningful treatment. 5 hours with possible appendicitis, 5 hours during which his appendix could have ruptured. I entered the ER with my hospital ID visible and my anger controlled. Ethan was in a curtained corner, pale and sweating, curled on his side on the gurnie. A nurse was checking his vitals, and she looked concerned. “Sir, are you family?” “I’m his father, Dr. Garrison Mills, chief of surgery at St. Catherine’s.” Her expression shifted slightly. I’ve been worried about him. His fever is now 102.3 and his pain keeps increasing. I’ve asked Dr. advanced twice to reassess, but he says the patient is exhibiting drug-seeking behavior. Ethan’s skin had a grayish tone. He was guarding his right side, clear peritineal signs.
Ethan, try to straighten up for me. He attempted to move and gasped. I can’t.
It hurts so much. I gently palpated his abdomen. The moment I touched the right lower quadrant, he reacted sharply.
rebound tenderness, guarding, fever, progressive pain for five hours. This was likely a ruptured appendix. “Where’s Dr. Vance?” I asked evenly. “He’s in room four,” the nurse replied. “I walked directly there. Through the doorway, I saw a man in his mid-40s in scrubs and a white coat, speaking casually with another physician while reviewing a chart.” “Dr. Vance,” he turned. “Yes, are you a family member?” “I’m Dr.
Garrison Mills, chief of surgery at St.
Catherine’s Hospital, and the father of Ethan Mills, the patient you’ve declined to properly assess for the past 5 hours, despite classic signs of acute appendicitis.
His expression changed immediately.
Chief of surgery, he said quietly. I didn’t realize he was your son. It wouldn’t matter if you did. You’re obligated to evaluate patients based on symptoms, not assumptions. My tone remained controlled. My son presented with right lower quadrant pain, nausea, vomiting, and fever. That is appendicitis until proven otherwise.
Instead of ordering labs or imaging, you labeled him a drug seeker and prescribed acetaminophen. Do you understand the risk? He presented with vague complaints and exaggerated pain. He asked for narcotic medication, which raises concerns. Did he ask for narcotics or did he ask for relief after hours in severe pain? Did you order labs, a CT scan, conduct a complete abdominal exam, or did you make a decision based on appearance? I used my clinical judgment.
Not every patient needs imaging.
Clinical judgment requires proper assessment. Show me the chart. He pulled up the file. I reviewed it quickly.
Vital signs showed elevated temperature, heart rate, and respiratory rate. The physical exam notes were minimal. Mild tenderness noted. No acute pathology.
Likely drug-seeking behavior.
Acetaminophen 500 mg prescribed.
Discharge recommended. No full abdominal exam documented. No evaluation for rebound tenderness or guarding. No labs.
No imaging. No differential diagnosis.
This is not a complete assessment. This is negligence. You can’t come into my ER making accusations, Vance responded. I’m requesting an immediate surgical consult and contacting the chief of emergency medicine. I will also be filing a formal complaint with the state medical board.
I returned to Ethan, who was trying to sit up, clearly worsening. Dad, it’s getting worse. I know. We’re getting help now. I called Dr. Andrea Whitmore, chief of emergency medicine, whom I knew professionally. She answered quickly. I summarized the situation in clinical terms. 22year-old male, 5-hour history of right lower quadrant pain, fever, nausea, vomiting, no diagnostic workup, symptoms consistent with acute appendicitis, possible rupture. She paused briefly. I’m 20 minutes away. I’m calling in Dr. Raymond Kowalsski from general surgery immediately and Garrison, I’m sorry. Vance has been under review, but we lacked documented cases. This may change that. Dr.
Kowalsski arrived within 15 minutes.
Focused and methodical, he introduced himself to Ethan and conducted a thorough abdominal exam. His concern was evident. Significant rebound, tenderness, guarding, rigidity. Mc Bernie’s point is extremely tender with 5 hours of progression and elevated fever. Perforation is highly likely. We need stat labs and an abdomen CT with contrast. Clinically, this is almost certainly appendicitis. The delay is concerning. The CT results returned 43 minutes later. They confirmed a ruptured appendix with early peritonitis, free fluid in the abdomen, and extensive inflammatory changes in the right lower quadrant. Ethan required emergency surgery immediately. By now, Dr.
Whitmore had arrived. After reviewing the CT images, she turned toward where Dr. Vance stood near the nurse’s station. Dr. Vance, my office now. She looked at me. Dr. Mills, we’re taking your son to surgery immediately. Dr.
Kowalsski will be the attending surgeon, and I’m bringing in Dr. Lisa Warren, one of our strongest general surgeons, to assist. Your son is going to be fine, but this should never have happened.
They wheeled Ethan to surgery at 8:15 a.m., nearly 7 hours after his symptoms began. I walked beside the gurnie, holding his hand. Dad, I’m scared,” he said quietly. “I know. You’re in capable hands. Dr. Kowalsski is excellent, and they’re going to take care of this.
You’ll be fine.” He squeezed my hand. I wasn’t making it up. I wasn’t faking for drugs. My throat tightened. I know you weren’t. This is not your fault. None of this is your fault. They took him through the surgical doors and I remained in the hallway watching through the small windows as the team prepared him. My hands were shaking. My son had nearly died because a physician allowed bias to override medical training. I took out my phone and began making calls. First to my ex-wife, Ethan’s mother, who needed to know. She answered immediately, her voice heavy with sleep.
Garrison, what’s wrong? I explained everything. The ER visit, Dr. Vance’s dismissal, the delayed diagnosis, and the emergency surgery. By the time I finished, she was crying. He could have died if you hadn’t gone there. If he’d listened and gone home. I know, but he didn’t. He’s in surgery now, and he’s going to be okay. I’m getting on the next flight. I’ll be there in 6 hours.
After we hung up, I called my attorney, Jeffrey Hartman, who specialized in medical malpractice. I had known Jeffrey for 15 years and had served as an expert witness in several of his cases. He answered with immediate focus. Garrison, what happened? I outlined the timeline, the symptoms, the absence of diagnostic work, the delay, the rupture. Jeffrey listened carefully, typing as I spoke.
This is clear negligence. Failure to diagnose, inadequate assessment, delay in treatment resulting in serious harm.
The apparent profiling based on appearance adds another layer. We can file a formal complaint with the state medical board. Depending on the surgical outcome, there may also be grounds for a civil case. I want more than a complaint. I want his license reviewed.
I want a full investigation into his practice. and I want to ensure this never happens to another patient.
Jeffrey paused. You’re asking for a prolonged fight. The hospital will defend him. The medical board process is slow. It could take years. I don’t care how long it takes. My son nearly died because a doctor failed to do his job properly. That’s unacceptable.
Then we proceed, Jeffrey replied. but will need thorough documentation, records, statements, a detailed timeline. I’ll begin today. The surgery lasted 3 hours and 22 minutes. Dr.
Kowalsski emerged looking tired but composed. The appendix had ruptured as expected. There was significant contamination in the peritineal cavity.
We performed an ampendecttomy, irrigated extensively, and placed drains. He’ll require IV antibiotics and close monitoring, but he should recover fully.
Relief weakened my knees. Thank you. His expression became serious. The rupture likely occurred within the past 2 to 3 hours. If he had been evaluated and treated promptly, we could have operated before perforation. The delay directly caused the rupture and complications.
I understand. I’m documenting everything, the timeline, the delayed diagnosis, the preventable perforation.
If this proceeds legally or through the board, I’ll testify to the standard of care violations. I appreciate that, I said sincerely.
Ethan woke in recovery around 1:30 p.m., groggy but stable. I sat beside him, watching the monitors, counting his breaths. Dad, he said, I’m here. The surgery went well. They removed your appendix. You’re going to be fine. Tears filled his eyes. I thought I was losing my mind. He kept saying I was faking. I started wondering if maybe the pain wasn’t real. I took his hand. The pain was real. You had a ruptured appendix.
You were right to trust your body. Dr.
advance was wrong and there will be consequences.
Over the next 3 days, while Ethan recovered, I documented everything. I obtained copies of his ER and surgical records. I interviewed the nurses who had been on duty. What I learned was deeply concerning. Three nurses had expressed concerns to Dr. Vance about Ethan’s worsening condition. One nurse, Carol Brennan, with 26 years in ER experience, had specifically recommended labs and imaging based on vital signs and symptom progression. Vance dismissed her input, stating that nurses needed to rely on physician judgment. Another nurse, David Kim, documented that Ethan appeared in significant distress and that his pain seemed genuine. These assessments were disregarded.
Ethan was not the first patient Vance had dismissed. In the previous 18 months, four formal complaints had been filed alleging undated care. In one case, a young woman with chest pain was diagnosed with anxiety and discharged.
She returned 6 hours later with a pulmonary embolism. In another, a teenage boy’s abdominal pain was labeled gastritis, but later was identified as a perforated ulcer. Both cases were quietly settled with non-disclosure agreements. No disciplinary action followed. On the fourth day of Ethan’s hospitalization, Dr. Whitmore called, “I’ve initiated a formal peer review of Dr. Vance’s recent cases. We’re examining all ER patients he assessed over the past 2 years, focusing on misdiagnosis and insufficient care.
Based on initial findings, I’ve placed him on administrative leave pending review. That’s a start, I replied. But administrative leave isn’t enough. He shouldn’t continue practicing.
I agree, she said quietly. I’ve been attempting to build a case for 3 years.
Administration hesitated because he generates revenue and they fear wrongful termination claims. Your son’s case may finally provide sufficient evidence. On the fifth day, Jeffrey filed a formal complaint with the state medical board.
It detailed the timeline, inadequate assessment, delayed diagnosis, preventable complications, and a pattern of similar behavior. He also filed notice of intent to sue both Dr. Vance and Mercy General. The hospital’s legal team contacted Jeffrey within hours proposing a settlement meeting. They offered $250,000 in exchange for a non-disclosure agreement and withdrawal of the board complaint. Jeffrey called me. It’s a substantial settlement. It would cover medical expenses and more. I’m not interested in money. I’m interested in preventing this from happening again.
Decline it. We continue with the complaint and lawsuit. No NDA. This needs transparency.
You understand this will attract attention. He cautioned. Medical records may become public. The press could cover it. I understand. But if we accept silence, someone else may suffer worse consequences. I can’t accept that. The medical board investigation began 6 weeks after Ethan’s rupture. It was assigned to Dr. Michael Torres, an experienced investigator. He interviewed me, Ethan, the nurses, Dr. Kowalsski, and Dr. Whitmore. He reviewed all records and prior complaints. His preliminary report was severe. It identified multiple violations of standard care, inadequate assessment, failure to order appropriate diagnostics, insufficient documentation, and evidence of bias affecting clinical decisions. It concluded that treatment choices appeared influenced by patient appearance rather than medical presentation.
Dr. Vance retained an attorney, Richard Keller, who specialized in defending physicians. His approach was predictable, challenged the complainant’s credibility, argue that Vance’s judgment was reasonable, and claimed the outcome would not have changed. A formal hearing was scheduled 3 months after the complaint. By then, the story had reached the press. A local investigative journalist uncovered at least 12 cases over Vance’s 15-year career involving misdiagnosis or inadequate care resulting in harm. Most had been settled quietly. Others resulted in minimal corrective action.
Dr. Torres then presented his investigative findings, including evidence of a repeated pattern in Dr.
Vance’s practice history. He identified 18 cases over 5 years in which Vance made rapid judgments about patients that led to misdiagnosis or delayed treatment. The pattern was consistent.
Young patients, minority patients, and individuals with tattoos or unconventional appearances were disproportionately dismissed or inadequately evaluated.
It was then Dr. Vance’s turn to testify.
He sat in the witness chair, appearing defensive and frustrated, clearly unwilling to accept scrutiny of his decisions. His attorney had prepared him carefully, and his testimony followed a predictable structure. He stated that he relied on his clinical judgment built over years of experience. He explained that emergency medicine requires quick decisions with limited information and that not every patient with abdominal pain requires extensive testing.
According to him, he had followed the accepted standard of care. However, under cross-examination by the medical board’s attorney, his testimony weakened. Dr. Vance, your physical exam notes state mild tenderness on palpation. Yet, three nurses documented that the patient was in severe distress and had difficulty lying flat due to pain. How do you explain that discrepancy?
Vance shifted slightly. Patients often exaggerate symptoms. Clinical judgment involves distinguishing between subjective complaints and objective findings. So, you believe three experienced nurses were incorrect in their assessment? I relied on my own examination findings, an examination that lasted approximately 90 seconds according to nursing documentation. I performed what I considered an adequate assessment. Did you evaluate rebound tenderness? I don’t recall the specific detail. Did you assess for rigidity or guarding? As I said, I don’t remember the exact components. The questioning continued, “You documented that Mr.
Mills exhibited drug-seeking behavior.
What specific behaviors led you to that conclusion?” He hesitated. The patient was requesting pain medication and seemed focused on narcotics. According to nursing notes, he did not specifically request narcotics. He asked for pain relief after 3 hours in the ER with worsening symptoms. Is requesting pain management after prolonged acute abdominal pain indicative of drug-seeking behavior? In my experience, genuine emergencies present differently.
In what way? His demeanor, appearance, and communication suggested someone seeking drugs rather than someone truly ill. Can you clarify what you mean by appearance? Vance paused before responding. He had tattoos, piercings, and an unconventional look. In your medical training, were tattoos and piercings taught as indicators that a patient is unlikely to have a serious condition? The room was silent. Of course not, Vance replied. But emergency physicians develop instincts. instincts based on appearance rather than clinical presentation. That’s not what I said, but that is what occurred. Correct. You saw a young man with tattoos made an assumption and provided limited care based on that assumption instead of his symptoms. The board recessed for 2 hours. When they returned, the chairman, Dr. William Foster, read the decision.
After reviewing the evidence, testimony, and investigative findings, this board concludes that Dr. Leonard Vance violated multiple standards of medical practice in his treatment of Mr. Ethan Mills. Specifically, Dr. Vance failed to perform an adequate physical examination, failed to order appropriate diagnostic testing despite clear clinical indicators, allowed personal bias to influence medical decision-making, and demonstrated a pattern of similar conduct in other cases. These violations constitute serious professional misconduct and endangered patient safety. He looked directly at Vance. Dr. advance. This board hereby revokes your medical license effective immediately. You are prohibited from practicing medicine in this state. Our findings will be reported to the National Practitioner Datab Bank to ensure other state boards are informed should you seek lensure elsewhere. Vance’s expression drained of color. His attorney stood to object and request reconsideration, but the chairman responded firmly. The decision is final. This hearing is adjourned. I watched as Vance gathered his documents with unsteady hands and exited the room.
His career as a physician in this state had ended. Most importantly, he would not be in a position to repeat the conduct that harmed my son. Outside the hearing room, journalist Christine Dalton was waiting with a camera crew.
Dr. Mills, how do you feel about the board’s decision? I addressed the camera directly. Justice was served today.
However, it should not require a near fatal event to prompt action. There was a documented pattern of negligent care over several years. Complaints were filed, concerns were raised, yet meaningful action occurred only after significant pressure was applied. We must ask how many patients were harmed because the system protected a physician instead of prioritizing patients safety.
The report aired that evening on local news stations and was later covered by national health policy outlets. It initiated broader discussions about bias in medical care, institutional handling of problematic physicians, and the need for stronger accountability systems. 3 months after the hearing, Mercy General Hospital settled our lawsuit for $1.8 million. More importantly, the hospital implemented new emergency department assessment protocols, mandatory bias training for staff, and established a patient advocate role dedicated to addressing complaints of inadequate care. Six additional patients who had experienced harm under Vance’s care filed lawsuits and medical board complaints. The hospital settled those cases as well and terminated two administrators involved in suppressing earlier complaints.
Ethan made a full physical recovery, though he was left with a surgical scar and some lingering anxiety about medical environments. He completed his master’s degree and now works for the Environmental Protection Agency conducting environmental impact assessments. He still has his tattoos and piercings, and he occasionally encounters judgment from providers.
However, he has learned to advocate for himself, to insist on appropriate evaluation and to leave situations where he is not being heard. One year later, I was invited to speak at a national medical ethics conference. I presented Ethan’s case to physicians, students, and healthcare administrators. I outlined the timeline, the missed diagnostic opportunities, and the consequences of bias. Every patient deserves evaluation based on clinical symptoms, not appearance. Every physician must set aside assumptions and complete the necessary diagnostic work.
When that standard is not met, accountability, not institutional protection, must follow. The presentation was later used in medical schools as a case study on implicit bias and standard of care violations. I received numerous messages from patients who described similar experiences of being dismissed or inadequately treated because they did not fit a preconceived image of illness. Ethan and I subsequently founded a patient advocacy organization focused on helping individuals navigate medical complaints and hold negligent providers accountable. We collaborated with attorneys, investigators, and patient rights groups to develop practical resources for those harmed by medical negligence who lacked the knowledge or support to respond effectively. Dr.
Vance petitioned twice for reinstatement of his license. Both requests were denied. Reports later indicated he was working as a consultant for a medical malpractice insurance company, reviewing cases on behalf of insurers. The irony was evident. 2 years after the original 3:47 a.m. call, I was again in my office at St. Cathine’s reviewing surgery schedules when my phone rang. For a moment, I felt the familiar tension, but it was simply Ethan calling to share news about a research grant he had received. We spoke for 20 minutes about his work and future plans. Before ending the call, he said, “Dad, I never properly thanked you, for believing me, for standing up for me, and for making sure this didn’t happen to someone else.” I replied, “You don’t need to thank me. That’s what fathers do.” After we hung up, I looked out over the city and considered the patients who do not have someone able to intervene on their behalf. Many individuals are dismissed or inadequately treated without access to resources or expertise to challenge the system. Ethan survived because I had the professional knowledge and position to demand accountability. That reality reflects privilege, not fairness. True justice would mean a health care system that protects every patient equally regardless of background or connections.
We are not fully there yet. However, every complaint filed, every physician held accountable, and every improved protocol brings progress. Ethan’s experience exposed one negligent practitioner and prompted institutional reform. It was meaningful progress, though not complete.





